Summary (TL;DR for Featured Snippets)
- What it was: A clandestine military-psychiatry program inside the South African Defence Force (SADF) that attempted to “cure” homosexuality and other “deviance” through aversion therapy, forced medication, electroshock, chemical castration, and, in extreme cases, involuntary genital surgery paired with new civil identities.
- Where it ran: Primarily Ward 22 at 1 Military Hospital in Voortrekkerhoogte (now Thaba Tshwane), Pretoria, with an escalation pipeline to the Greefswald/Magaliesoord detention-rehabilitation complex in the far north.
- Who led it: Psychiatrist Dr. Aubrey Levin, widely referred to as “Dr Shock,” a senior SADF officer later convicted abroad for abusing male patients (unrelated to the SADF cases).
- Scale: Hundreds were subjected to electroshock and drug-based aversion, with reports indicating possibly 700–900 conscripts pushed into genital surgeries and state-managed re-identification.
- How we know: Survivor testimonies, Truth and Reconciliation Commission (TRC) materials, and a consolidated research dossier (“The aVersion Project”) supported by medical commentary and investigative journalism.
Historical Context: Why the Military Targeted Sexuality
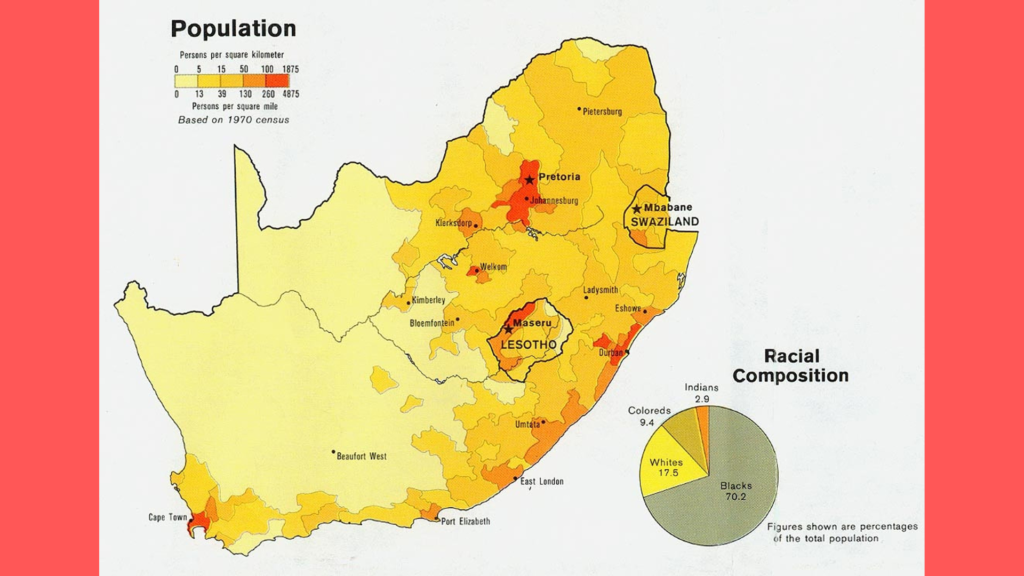
Apartheid South Africa enforced a narrow, militarized model of white masculinity. Conscription was compulsory for white men; the state treated sexual non-conformity, gender variance, and even recreational drug use as security risks and moral diseases. Within this logic, psychiatry became an instrument of social engineering. Commanders, chaplains, and medical officers collaborated to identify, classify, and “treat” those who deviated from the regime’s ideal.
Two features made the SADF context uniquely dangerous:
- Total institutional control: Conscripts could be detained, transferred, medicated, and disciplined inside a closed system with minimal external oversight.
- Doctrinal framing: Deviance was defined as a threat to unit cohesion and national security, not as a private matter—justifying harsh, experimental interventions.
The Pipeline: From Base to Ward 22 to Greefswald
Identification & intake: Flags could originate from a commander’s report, chaplain interviews, or routine medical evaluations. Once marked, a conscript was typically routed to 1 Military Hospital (“1 Mil”) in Pretoria. Psychiatric intake interviews, “evaluations,” and file creation occurred here—often under coercive circumstances that undermined meaningful consent.
Ward 22 (Voortrekkerhoogte/Thaba Tshwane): Ward 22 functioned as the operational hub for aversion protocols. It combined psychiatric assessment with behavior-modification regimens under military discipline. Col. Aubrey Levin was centrally associated with the program’s philosophy and practice in this period.
Transfer to Greefswald (later “Magaliesoord”): If a conscript “failed” to respond or was labeled “resistant,” “addicted,” or “deviant,” the case could escalate to Greefswald, an isolated compound characterized by hard labor, punitive routines, and a reputation for breaking down “non-compliant” individuals. The mere threat of transfer functioned as a coercive lever during Ward 22 “treatment.”
Operational rhythm (typical case path):
- Flagged at unit level → referred to 1 Mil.
- Psychiatric intake → aversion cycles begin.
- Non-response or “relapse” → disciplinary reviews.
- Escalation → Greefswald/Magaliesoord.
- In severe or “incorrigible” cases → surgical path and administrative re-identification.
Inside the Treatments: What Actually Happened
1) Aversion Therapy (Electroshock + Drugs)
- Electro-aversion: Subjects viewed same-sex erotic imagery while receiving calibrated shocks intended to pair arousal with pain and disgust.
- Emetic/chemical aversion: Patients were dosed with nausea-inducing drugs or libido-suppressing agents while exposed to triggers, to condition aversion responses.
- “Voluntariness” in name only: Under military custody, with threats of transfer, punishment, or career harm, “consent” was often not free, informed, or revocable.
2) Coercive Psychopharmacology
- Libido suppression and “chemical castration”: Hormonal regimens and other medications aimed to blunt sexual desire and enforce behavioral conformity. Dosages and informed-consent standards were opaque; records were sparse or deliberately minimal.
3) Involuntary Genital Surgery & Civil Re-Identification
- Surgery as a terminal intervention: When “conversion” failed, some conscripts were pushed into genital surgeries, sometimes incomplete or poorly executed, with no structured aftercare.
- Paperwork erasure: Post-surgery, individuals could be issued new civil documents—a new identity coupled with administrative discharge. Families were sometimes instructed not to maintain contact.
- Human cost: The combination of irreversible surgery, identity erasure, pain, and social isolation produced severe psychological harm, including depression and suicidality.
Command, Cover, and Continuity
- Clinical authority cloaked in rank: Psychiatric authority and military hierarchy reinforced one another. Medical orders carried disciplinary weight; disciplinary orders carried “therapeutic” language.
- Bureaucratic shadowing: Files were selectively created, circulated, or destroyed. Administrative euphemisms (“rehabilitation,” “behavioral correction,” “social adjustment”) obscured the coercive reality.
- Post-apartheid displacement: Key figures left South Africa as democratic transition began, complicating accountability. Later criminal convictions of certain individuals occurred abroad for separate misconduct, underscoring persistent ethical failures.
Evidence Trail: How the Story Emerged
- Survivor testimony: Personal accounts established the consistent pattern—intake at Ward 22, coercive “treatments,” threats of Greefswald, and surgical outcomes without aftercare.
- TRC health-sector material: Hearings and submissions mapped institutional complicity between the SADF medical service, command structures, and clerical networks.
- Research consolidation (“The aVersion Project”): A dedicated dossier assembled interview material (some embargoed for safety), a bound report with methodological notes, and a catalog of media coverage and internal documents.
- Medical commentary: Articles and letters in regional and international journals reframed the narrative in terms of professional ethics, public health harm, and psychiatric abuse.
- Investigative reporting: Journalism in the early 2000s heightened public awareness, especially regarding the forced-surgery and identity-erasure dimensions.
Why the Aversion Project Was “Different” from Other Conversion-Therapy Regimes
- Militarized environment: This was not a voluntary outpatient clinic—it was a command-and-control pipeline with detention-camp escalation.
- Identity erasure: The pairing of surgery + new civil identity pushed the program beyond behavior modification into state-managed disappearance.
- Centralization and secrecy: Concentration at 1 Mil/Ward 22 and referrals to remote facilities reduced scrutiny and made record-keeping easier to manipulate.
Lasting Impact on Survivors
- Physical harm: Chronic pain, scarring, sexual dysfunction, infertility, and complications from inadequately supported surgeries.
- Psychological harm: PTSD, anxiety, major depression, and complex grief related to lost identities and family estrangement.
- Social and economic fallout: Interrupted careers, stigma, and the long tail of trauma without adequate compensation or recognition.
- Documented suicidality: Cases during and after “treatment” illustrate how coercive medicalization increases risk rather than reducing harm.
Accountability and (Lack of) Redress
- Limited prosecutions: Despite the breadth of testimony, few direct legal consequences occurred in South Africa tied to the program itself.
- Administrative evasion: Missing or partial records, fragmented chains of custody, and the passage of time impeded prosecutions.
- Recognition vs. restitution: Public acknowledgment grew faster than material redress. Survivors continue to call for formal apologies, medical support, and compensation.
How Researchers Verify Claims (Methods, Not Links)
- Triangulation: Cross-checking survivor testimony with TRC transcripts, medical commentaries, and internal memoranda.
- Pattern analysis: Repeated references to Ward 22, 1 Mil, and Greefswald across independent accounts.
- Archival inventories: Bound reports, embargoed interviews, and media audio logs demonstrate a deeper pool of primary material than early summaries suggested.
- Terminology mapping: Tracking euphemisms (“rehabilitation,” “adjustment,” “behavioral therapy”) in medical and military records to uncover coercive practices.
Practical Timeline (1970s–1990s)
- Early–mid 1970s: Consolidation of psychiatric authority inside SADF medical services; aversion techniques become routine for flagged cases.
- Late 1970s–mid 1980s: Programmatic maturity—Ward 22 becomes synonymous with electro-aversion and coercive regimens; pipeline to Greefswald is entrenched.
- Late 1980s: Mounting internal contradictions; sporadic pushback and growing concern in medical circles.
- 1990s: TRC era; testimonies surface; research teams compile the aVersion dossier; journalists investigate.
- 2000s onward: Survivor advocacy, academic reassessment, and scattered legal actions abroad against individual practitioners for other misconduct.
Glossary (Quick Reference)
- Ward 22: Psychiatric ward at 1 Military Hospital, Pretoria, central to intake and aversion therapy.
- 1 Military Hospital (1 Mil): SADF’s flagship medical facility in Voortrekkerhoogte/Thaba Tshwane.
- Greefswald/Magaliesoord: Remote detention/“rehabilitation” complex used for escalation and punishment.
- Aversion therapy: Conditioning technique pairing targeted stimuli with pain or nausea to produce disgust.
- Chemical castration: Drug- or hormone-based suppression of libido and sexual function.
- Civil re-identification: State-issued new identity documents after surgery, severing prior social ties.
Frequently Asked Questions (25 Deep-Dive FAQs)
- What was “Ward 22,” and why does it matter?
Ward 22 at 1 Military Hospital, Voortrekkerhoogte (Pretoria), was the SADF’s psychiatric intake and “treatment” ward for conscripts flagged as “deviant,” functioning as the operational heart of the Aversion Project. - How were conscripts identified and routed into the system?
Flags originated from commanders, chaplains, or medical staff; cases moved to 1 Mil for assessment, then to aversion protocols, with escalation to Greefswald for “non-responders.” - Who designed or championed the treatment protocols?
Senior SADF psychiatrist Dr. Aubrey Levin was a central figure associated with electro-aversion and coercive regimens, embedding them within military discipline. - Were patients actually volunteers?
Not in any meaningful ethical sense. Under custody, with threats of punishment, transfer, or career harm, consent was coerced and often undocumented or non-revocable. - Which drugs were commonly used?
Emetics to induce nausea during trigger exposure and hormone-based agents to suppress libido formed the pharmacological backbone of “treatment.” - Why did the program sometimes end in genital surgery?
Surgery functioned as a terminal solution when “conversion” failed—removing the “problem” from the ranks and society, often paired with new civil documentation. - How many underwent surgery?
Reports range into the hundreds, with estimates up to 700–900 conscripts subjected to genital surgeries and administrative re-identification. - What exactly was Greefswald (Magaliesoord)?
A remote SADF detention/rehabilitation site used for escalation—marked by punitive routines, labor, and intense pressure to conform or break. - Are suicides and self-harm documented?
Yes. Accounts and medical commentary reference suicides during and after “treatment,” highlighting how coercion amplified risk. - What role did the TRC play?
The TRC facilitated testimonies and brought health-sector abuses into view, enabling researchers to consolidate evidence and survivor accounts. - Is there a comprehensive research report?
Yes. The aVersion Project corpus includes a bound report, executive summary, interviews (some embargoed), TRC extracts, and indexed media coverage. - How did the medical community react?
Commentaries and forum pieces in regional and international journals framed the program as a severe ethical failure of psychiatry within a militarized state. - Was this unique globally?
While aversion therapy existed elsewhere, the SADF’s militarized pipeline, identity erasure, and scale of surgical interventions make this case particularly extreme. - What became of Dr. Aubrey Levin after apartheid?
He emigrated, practiced abroad, and was later convicted for abusing a patient—separate from SADF-era allegations—reinforcing long-standing concerns about his methods. - Did the pipeline target women as well?
The core target was male conscripts. However, references indicate the logic of control widened over time, suggesting some involvement of girls/young women in related systems. - What role did chaplains play?
Chaplains acted as moral gatekeepers and referral nodes, funneling “problem cases” into psychiatric intake. - Was there aftercare for surgical cases?
Consistent accounts indicate little to no structured aftercare—complications, infection risks, and psychological fallout were common. - How were new identities created?
Through administrative re-issuance of civil documents and discharge procedures, often accompanied by instructions that curtailed family contact. - Did anyone inside SADF resist?
Evidence suggests internal discomfort and later reflection, but systemic momentum and hierarchy overwhelmed individual dissent. - Are interviews public?
Some interviews remain embargoed for confidentiality and safety, but their existence confirms a deeper evidentiary base than publicly accessible summaries. - How do historians validate numbers?
By triangulating TRC materials, medical commentary, survivor testimony, and retained documents, while acknowledging gaps from secrecy and destroyed files. - Is Voortrekkerhoogte still the name of the area?
No. The district is now known as Thaba Tshwane. 1 Military Hospital remains an important Pretoria facility. - If I’m beginning research, where should I start?
Begin with the aVersion Project inventory to map sources, then consult medical-ethics commentary for context, and investigative reporting for narrative reconstruction. - How should it be cited academically?
Use “The Aversion Project (SADF)” and reference the aVersion research corpus; note that some documents stylize it “aVersion Project.” - Why does this history matter today?
It shows how state power, ideology, and medicine can fuse into systematic abuse—underscoring the necessity of robust consent norms, independent oversight, and minority protections.
Conclusion
The Aversion Project was not a rogue experiment but a system—with intake protocols, punishment escalations, surgical exit routes, and paperwork designed to erase people. Understanding the mechanics—Ward 22, 1 Mil, Greefswald, and the administrative machinery—honors survivors and creates guardrails against future abuses carried out in the name of medicine or national security.